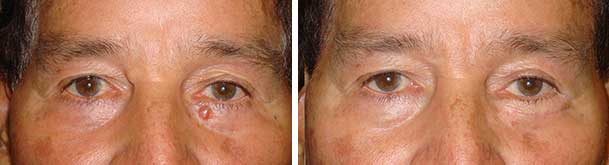
After being diagnosed with a basal cell skin cancer on my eyelid, Dr Taban was referred via my dermatologist. The day of my reconstruction he presented me with multiple options and pros and cons … We didn’t know how skin was going to be removed from my eyelid until I had my cancer removed the day before his surgery to reconstruct it. He’s a great surgeon and you cannot even tell that I had half a dime-sized piece of skin cut off my eyelid…
Jimmy Stegner
September 2017